
Members of the group stains violet in Gram stain. They are round or coccoid in shape but vary in formation. They are identified based on their possession of the enzyme catalase or their ability to produce hemolysis on culture medium or the ability to hydrolyze arginine.
1. The
Staphylococci
2. The
Streptococci
3. The
Anaerobic Cocci
4. The
Enterococci
5. The
Aerococci
THE STAPHYLOCOCCI
Characteristics:
1. They are non–motile, non–capsulated, non–spore formers gram positive cocci with grape–like cluster appearance.
2. They are facultative anaerobes or microaerophilic but grown best with oxygen.
3. They are catalase positive and slowly ferment carbohydrates to produce acid but not gas.
4. They can ferment glucose except Staphylococcus saphrophyticus.
5. They are resistant to drying, heat (even at 60oC for 30 minutes) and high salt concentration.
6. They can be isolated using Mannitol Salt Agar, a selective medium for the isolation of staphylococci.

|
DIFFERENTIAL
CHARACTERISTIC BETWEEN |
||
|
|
Staphylococcus
aureus |
Staphylococcus
albus |
|
Colonial pigmentation |
golden yellow |
porcelain white |
|
Coagulase |
positive |
negative |
|
Mannitol fermentation |
positive |
negative |
|
Lipase & Dnase |
positive |
negative |
|
Hemolysis |
beta–hemolytic |
negative |
|
Protein A |
present |
absent |
|
Teichoic Acid |
ribitol type |
glycerol type |
|
Glucose metabolism |
fermentative |
fermentative |
Antigenic structure:
1. Teichoic acid (TAs) – polysaccharide in nature. There are two types of TAs: lipo–TAs (LTA), which are anchored in the cytoplasmic membrane, and cell wall TAs (WTAs), which are covalently linked to peptidoglycan in the bacterial cell wall.
2. Protein A – protein in nature; anti–phagocytic.
Cultural characteristics:
1. In
broth – they produce uniform turbidity.
2. On
plates – colonies are opaque, circular, smooth with a butyrous consistency with
description of oil paint appearance.
3. On Blood Agar Plate (BAP) medium – they produce hemolysis which is beta– hemolytic.
Pathogenicity test for Staphylococcus aureus:
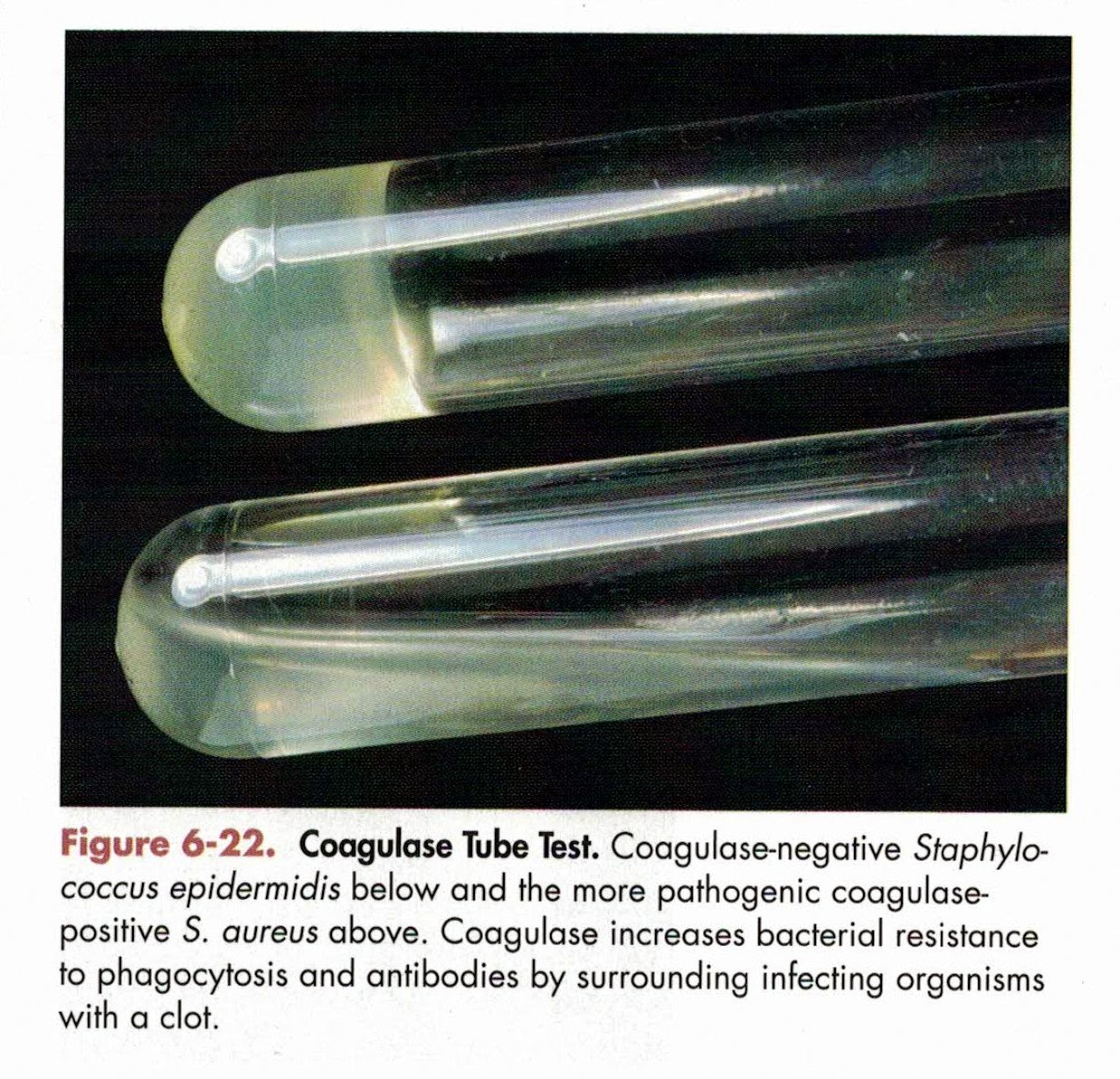
1. Coagulase test – best single criterion of pathogenicity of Staphylococcus aureus.
Based on the principle that the organism elaborates the enzyme coagulase which is capable of coagulating plasma and that is coagulase (+)
2. Growth on Tellurite medium – most coagulase Staphylococcus aureus release tellurite with a production of jet-black colony.

3. Mannitol fermentation test – pathogenic strains of Staphylococcus aureus ferments mannitol and tolerate relatively high concentration of salt which is 7.5 – 10% sodium chloride, aerobically and anaerobically.
Medium used: MSA – Mannitol Salt Agar
pH indicator – phenol red

(+) result –
yellow halo for S. aureus
– pink colonies for S. epidermidis
4. Staphylococcal Protein A (SpA) – differentiates pathogenic Staphylococcus from non–pathogenic staphylococcus. Pathogenic staphylococcus has Protein A on their cell wall, the non–pathogenic staphylococcus has Protein B in their cell wall. It binds to the Fc portion of all human IgG subclasses (except IgG3) therefore interferes with antibodies and complement deposition on the bacterial surface and thus resists phagocytosis.
5. Lysostaphin sensitivity – a rapid screening test to differentiate Staphylococcus aureus from other species of staphylococci and micrococci.
6. Alpha–hemolysin – it serves as an index of virulence because the more virulent the strain, the more alpha hemolysin is produced.
7. Ribitol in cell wall is present, like Staphylococcus aureus and Staphylococcus saprophyticus but not Staphylococcus epidermidis.
Enzymes produced by Staphylococcus aureus:
1. Coagulase – an enzyme–like protein which clots plasma.
2. Catalase – allows the bacteria to resist intra– and extracellular killing by hydrogen peroxide.
3. Nuclease – heat resistant, heating at 65oC causes structural disruptions but changes are reversible.
4. Gelatinase – breaks down amino acids and peptides to be transported inside the cell directly.
5. Staphylokinase (SAK) – a protease precursor with fibrinolytic activity (dissolves the clot formed). It plays a part in producing staphylococcal septicemia by dislodging infected intravascular thrombi.
6. Hyaluronidase (HysA) – known as the spreading factor. It splits hyaluronic acid thus spreading to the organism.
7. Phosphatase (PtpB) – PtpB was initially described as a tyrosine phosphatase, however recent phosphoproteomic analysis indicated that PtpB functions as an arginine phosphatase that is involved in oxidative stress response, amino acid metabolism, and virulence factor synthesis.
8. Dnase – hydrolyze DNA to be used as source of carbon and energy for growth and release free nucleotides and phosphate.
Toxins produced by Staphylococcus aureus:
Exotoxins are a group of soluble proteins that are secreted by the bacterium that enter host cells and catalyze the covalent modification of a host cell component(s) to alter the host cell physiology.
All toxins thus far identified share a number of important properties, including (1) an ability to cause emesis and gastroenteritis in a primate model, (2) superantigenicity, (3) intermediate resistance to heat and pepsin digestion, and (4) tertiary structural similarity (where known) including an intramolecular disulfide bond.
Superantigenicity refers to the ability of these exotoxins to stimulate proliferation of T–lymphocytes without regard for the antigen specificity of these cells.
1. Pyrogenic Toxin Superantigens (PTSAgs)
The molecular basis of PTSAg toxicity is presented in the context of two diseases known to be caused by these exotoxins: (a) Toxic Shock Syndrome and (b) Staphylococcal Food Poisoning (SFP) thus two toxins were identified:
a. Toxic Shock Syndrome Toxin–1 (TSST–1) – previously known as staphylococcal pyrogenic exotoxin C or staphylococcal enterotoxin F. It is responsible for essentially all cases of menstrual–associated toxic shock syndrome (TSS). It is characterized by high fever, rash, hypotension, multiorgan failure (involving at least 3 or more organ systems), and desquamation, typically of the palms and soles, 1–2 weeks after the onset of acute illness. The clinical syndrome can also include severe myalgia, vomiting, diarrhea, headache, and non–focal neurologic abnormalities. Also found in 60% of patients with Kawasaki syndrome.
b. Staphylococcal Enterotoxins (SEs)
Responsible for food poisoning. It is protein in nature and can withstand boiling for 30 minutes which may kill staphylococci but not the toxin. The effect is on the CNS vomiting center and neural GIT receptors. These are five antigenic types, the most important is type A Staphylococcus aureus produces enterotoxin while growing in meat, dairy or bakery products. The enterotoxins are absorbed in the gut.
2. Hemolysins & Leukocidin
Hemolysins produced by Staphylococcus aureus are toxic to the red blood cells while those which are toxic to the white blood cells are called leukocidin.
a. Alpha hemolysin or Alpha toxin – is a pore forming toxin that penetrates host cell membranes causing osmotic swelling, rupture, lysis and subsequently cell death. It dissolves rabbit, mice, and human red blood cells. It is both dermonecrotic and neurotoxic.
What was previously known as Neisser–Weschberg Leucocidin is now known as alpha hemolysin.
b. Beta hemolysin or Beta toxin – can produce “hot cold” lysis, which enables hemolytic activity if incubation at 37oC is followed by a period of 10oC less. It dissolves sheep red blood cells but not rabbit erythrocytes. It is also found to have phosphorylase C activity. This activity requires the presence of Mg2+ and is limited to sphingomyelin and lyso–phosphatidylcholine. The differing susceptibility of erythrocytes to beta-hemolysin may be due to the differing sphingomyelin contents of erythrocytes.
c. Delta hemolysin or Delta toxin – produced by 97% of S. aureus strains. It is also hypothesized that 50 to 70% of coagulase–negative staphylococci produce this toxin. Although delta–toxin causes a wide range of cytotoxic effects, its importance in disease etiology remains unclear. Delta–hemolysin is capable of lysing erythrocytes and other mammalian cells, as well as subcellular structures such as membrane-bound organelles, spheroplasts, and protoplasts. Also, dermonecrotic activity has been observed, as well as lethality in experimental animals when used in high concentrations. It remains possible, however, that these activities result from contamination with very small amounts of alpha toxin. The presence of phospholipids inhibits delta–hemolysin activity.
d. Gamma hemolysin or Gamma toxin & Panton Valentine Leukocidin – each of these toxins is made as two non–associated secreted proteins, referred to as S and F components.
Gamma–hemolysin is made by virtually every strain of Staphylococcus aureus, while PV leukocidin is made by 2 to 3% of strains. The toxins affect neutrophils and macrophages, and gamma–hemolysin is additionally able to lyse many varieties of mammalian erythrocytes. Gamma–hemolysin is not identifiable on blood agar plates, however, due to the inhibitory effect of agar on toxin activity.
Leukocidin or leukotoxins also known as Panton Valentine Leukocidin which attacks polymorphonuclear cells and macrophages and no other cell type and cause tissue necrosis and severe necrotizing pneumonia. It is one of the virulent genes expressed by Methicillin Resistant Staphylococcus Aureus (MRSA). Panton–Valentine leucocidin (PVL) is a toxin composed of two components, LukS–PV, and LukF–PV. These two components are secreted before they assemble into a pore–forming heptamer on neutrophil membranes, leading to neutrophil lysis.
3. Epidermolytic or Exfoliative Toxin (ET) – serine proteases secretion which causes toxic epidermal necrolysis or the so–called Scalded Skin Syndrome (a blistering skin disorder that particularly affects infants and young children).
Staphylococcal infections:
1. Staphylococcus aureus
a. Cellulitis,
boils, impetigo, acne, post–operative wound infection, furuncle or abscess
(prototype infection)
b. Food
poisoning
c. Septicemia, endocarditis, meningitis, puerperal sepsis, pneumonia, osteomyelitis, carbuncles, cystitis, peritonitis, and toxic shock syndrome in woman using tampoons.
2. Staphylococcus epidermidis
a. A
resident flora of the human skin becomes pathogenic if implanted to areas other
than skin. Common cause of acne, pimples, stich abscess, mild UTI,
endocarditis, bacteremia, meningitis
b. Coagulase
(–) and MSA (–)
c. Presence
of glycerol in cell wall.
d. Biotin is a requirement for growth.
3. Staphylococcus saphropyticus
a. Usually
isolated in urine of woman with UTI.
b. Resemble
S. epidermidis but can be distinguished by virtue of its resistance to
Novobiocin and Nalidixic Acid.
c. Ribitol is present in the cell wall.
4. Other staphylococcal species detected in human (Coagulase–negative Staphylococcus or CoNS)
a. Staphylococcus hominis – is commonly recognized as a contaminant on blood cultures being a part of normal skin flora, but on rare occasions, may also cause native valve endocarditis (NVE) with embolic phenomena.
b. Staphylococcus haemolyticus – causes severe infections in several body systems including meningitis, endocarditis, prosthetic joint infections, and bacteremia and is prevalent in the hospital environment and on the hands of healthcare workers. It is also known to cause septicemia, peritonitis, otitis media and diabetic foot ulcer (DFU) infections.
c. Staphylococcus simulans – infrequently been isolated as a causative agent for UTIs. It is an opportunistic pathogen among animals (cows, goats, horses, and other farm or domesticated animals) and has been frequently associated with bovine mastitis.
d. Staphylococcus cohnii – is found colonizing skin and mucosa. Nevertheless, there is little literature regarding its involvement in human infections. Cases of catheter–associated infection, meningitis, urinary infection, and cholecystitis have been reported, but it's cause of human disease is only 0.5% to 8%, as presented in different case series.
e. Staphylococcus warneri – is catalase positive, oxidase negative, coagulase negative organism, which is a commensal on skin flora. It constitutes <1% of skin Staphylococcus flora. It is a rare cause of sepsis, and an immunocompromised state is a predisposing factor for such infections. There are reported cases of catheter–related bacteremia, endocarditis, multiple abscesses, septic arthritis caused by Staphylococcus warneri. Isolates from these infections are generally resistant to Penicillins, with beta–lactamase activity and show susceptibility to other antibiotics with gram-positive activity. Infections due to these organisms were successfully treated with fluoroquinolones, among other antibiotics.
Laboratory diagnosis:
1. Gram staining – violet cocci in grape like cluster
2. Catalase test – produces bubbling reactions with H2O2.
3. Culture
|
Agar |
Colonies |
|
Mannitol Salt Agar (MSA) |
Yellow colonies |
|
Baird–Parker Agar aka Egg Tellurite–Glycine–Pyruvate
Agar (ETGPA) |
Dark gray to black, shiny, medium–sized colonies,
clear halos surrounding colonies |
|
Vogel Johnson Agar aka Tellurite Glycine Agar |
Black, convex shiny colonies surrounded by a
yellow zone |
4. Pathogenicity Test
Phage typing is
based on susceptibility of the staphylococci to symbiotic bacteriophage due to
their surface receptors. Lysogenic strains are those which are lysed by one or
more specific bacteriophage. It is indicated by the presence of a clear zone around
the bacteriophage. It is of value in investigating the exact strains which may
cause epidemic outbreaks.
THE STREPTOCOCCI
They are widely distributed in nature and maybe found in milk and dairy products, water, dust, vegetation, normal respiratory tract of various animals including humans.
Characteristics:
1. They are fastidious (organisms that require many growth factor) requiring enriched media like BAP for growth.
2. They are gram (+) cocci arranged in chain, division in plane is perpendicular to the long axis of the chain.
3. They are catalase negative. Most are facultative anaerobes; some strains require 10% CO2 for initial isolation. Only the peptostreptococci group are obligate anaerobes.
4. Some strains have capsules composed of hyaluronic acid.
5. They have a small, pinpoint, translucent to opaque, circular colonies and appear as minute beads of moisture. Some strains exhibit hemolysis.
6. Colony variation is quite common: mucoid, matte, or rough (has large amount of M–protein), smooth or glossy (contains little amount of M–protein)
7. They are non–motile, non–sporeforming, non–encapsulated except members of Group A,B,C,D are encapsulated.
Antigenic structure:
1. Hyaluronic acid – similar to staphylococci.
2. M–protein – forms the basis of the virulence of streptococci and serologic typing. It may be involved in rheumatic fever where streptococcal antigen cross reacts with cardiac connective tissue protein.
3. Carbohydrate (C–carbohydrate or group specific substance) – used by Lancefield as the basis for streptococcal grouping.
Classification of Streptococci:
A. Academic or Bergey’s Classification – a classification based on physiological and biochemical characteristics:
1. Pyogenic group – pus forming organism which grows at neither 10oC nor at 45oC. They cause streptococcal pharyngitis and scarlet fever.
2. Viridans Group Streptococci (VGS) – a normal flora of the human respiratory tract and cause disease only when they settle on another site. Grows best at 45oC but not at 10oC. Today, the VGS are classified into 6 major groups:
a. Streptococcus mutans group
The natural habitat of Streptococcus mutans is the human oral cavity, more specifically the dental plaque, a multispecies biofilm formed on hard surfaces of the tooth. As a human pathogen Streptococcus mutans is also implicated in sub–acute bacterial endocarditis, a life-threatening inflammation of heart valves, while a subset of strains has been linked to other extraoral pathologies such as cerebral microbleeds, IgA nephropathy and atherosclerosis. Strains of S. mutans can be classified into four different serological groups (c, e, f and k) based on the composition of cell-surface rhamnose–glucose polysaccharide.
b. Streptococcus salivarius group
This group consists of three genetically similar species, Streptococcus salivarius, Streptococcus vestibularis and Streptococcus thermophilus.
Streptococcus salivarius and Streptococcus vestibularis are commensal organisms that may occasionally cause opportunistic infections in humans, whereas Streptococcus thermophilus is a food bacterium widely used in dairy production.
c. Streptococcus mitis group
The Streptococcus mitis group is comprised of 13 species including some of the most common human oral colonizers such as Streptococcus mitis, Streptococcus oralis, Streptococcus sanguinis and Streptococcus gordonii as well as species such as Streptococcus tigurinus, Streptococcus oligofermentans and Streptococcus australis that have only recently been classified and are poorly understood at present.
d. Streptococcus sanguinis group
Streptococcus sanguinis is an abundant oral commensal which can cause disseminated human infection if it gains access to the bloodstream. The most important among these diseases is infective endocarditis (IE). Infective endocarditis occurs when microorganisms enter the bloodstream and colonize the cardiac endothelium.
e. Streptococcus anginosus group (See Group C Streptococci below)
f. Streptococcus bovis group (See Group D Streptococci below)
Facklam in 2002 introduced a short, reliable biotyping scheme with six tests for the classification and identification of VGS which includes the production of acetoin, fermentation of mannitol and sorbitol, hydrolysis of arginine, esculin and urea.
3. Enterococcus group – current scheme of classification now recognized a new genus Enterococcus. They grow best at 10oC and 45oC and withstand temperatures above 60oC, so they are heat resistant. All species of this group give alpha or gamma reaction on sheep BAP except Streptococcus fecalis which is beta hemolytic.
4. Lactic group – harmless group of streptococci which is present in milk and are often responsible for the normal coagulation or “souring” of milk.
5. Peptostreptococci – strict anaerobes, occur in normal flora of the gut and female genital tract. (Details below on GPAC or Gram–positive Anaerobic Cocci)
B. Smith and Brown’s Classification – a classification based on the reaction on BAP; hemolysis
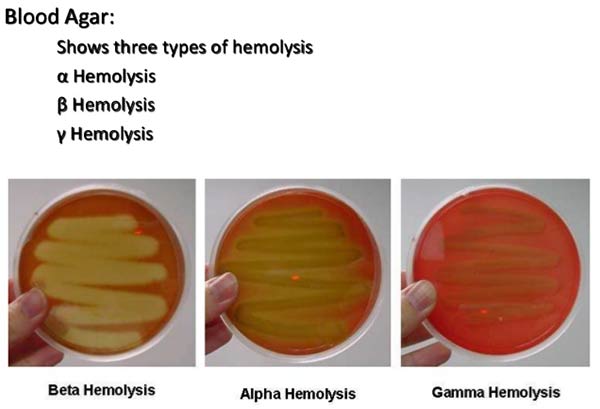
1. Alpha hemolytic streptococcus or green streptococcus – produces incomplete hemolysis of RBC accompanied by a greenish or brownish discoloration possibly due to methemoglobin. This group forms long chains especially when grown in liquid media.
Streptococcus pneumoniae
Alpha prime – there is a small zone of hemolysis surrounding the colony with an extension of a zone of complete hemolysis.
2. Beta hemolytic streptococcus – produces clear, colorless zone around the colony indicating complete lysis of the RBC. Colorless zone of hemolysis is due to lysis of the RBC by the streptococci releasing hemoglobin which diffuses into the medium.
Streptococcus
pyogenes
Streptococcus agalactiae
3. Gamma hemolytic streptococcus – no apparent hemolysis
C. Lancefield classification – a classification based on the presence of a specific carbohydrate antigen known as C–polysaccharide.
1. Group A – predominantly pathogenic to man; most of which are beta hemolytic.
Streptococcus pyogenes
a. Local and invasive form
(1) Pharyngitis
/ Tonsilitis (streptococcal sore throat)
(2) Skin
and soft tissue infection (erysipelas)
(3) Septicemia
b. Post–streptococcal sequela
(1) Rheumatoid
fever (cell membrane antigen of streptococci cross react with heart sarcolemma)
(2) Acute glomerulonephritis
c. Quinsy, Ludwig’s angina
For primary isolation of Streptococcus, sheep blood is preferred for Blood Agar Plate because it has inhibitory effect to the growth of Hemophilus haemolyticus, an organism which resemble streptococcus in its colonial morphology and beta hemolytic reaction.
Test for Group A Streptococci:
a. Bacitracin Disk Test – primarily for pharyngeal culture, a useful presumptive test for differentiating Group A beta hemolytic streptococci.

Based on the principle that growth of Group A beta hemolytic streptococci is inhibited by a paper disc containing 0.04 units of Bacitracin (Taxo A). In this test, regardless of measuring the zone, is already positive.
b. PYR Test
Based on the detection of pyrrolidonyl peptidase (PYRase) activity of Enterococcus specie and Streptococcus pyogenes. Broth culture after 4 hours incubation was added with L–Pyrrolidonyl–β–naphthylamide (PYR reagent). A positive result is the development of bright cherry red color.

2. Group B Streptococci: Streptococcus agalactiae
a. Normal
flora of the female genital tract and an important cause of neonatal sepsis and
meningitis. Normal flora of GIT and pharynx.
b. Produce
small zones of beta hemolytic on sheep blood. The colonies are large and mucoid.
c. Give
positive result to CAMP test (Christie, Atkins, Munch–Petersen)
d. Rarely
Bacitracin positive
e. In
liquid media, they tend to grow as diplococci or in short chains.
f. A
double zone of hemolysis on rabbit blood agar may be observed when the blood is
refrigerated after initial incubation.
g. Produces yellow, red, or orange pigment and the pigment production is suppressed if glucose is added to the medium used.
Test for Group B Streptococci:
a. Hippurate Hydrolysis Test
Hippurate hydrolysis relies on the ability of the enzyme called hippurate hydrolase produced by microorganisms to hydrolyze sodium hippurate to benzoic acid and glycine. This test does not require microorganisms to grow, but instead it detects the presence of already formed enzymes by testing for glycine, one of the end products of hydrolysis. If glycine is present a blue or deep purple color is formed. All Lancefield Group B streptococci are positive for hippurate hydrolysis.

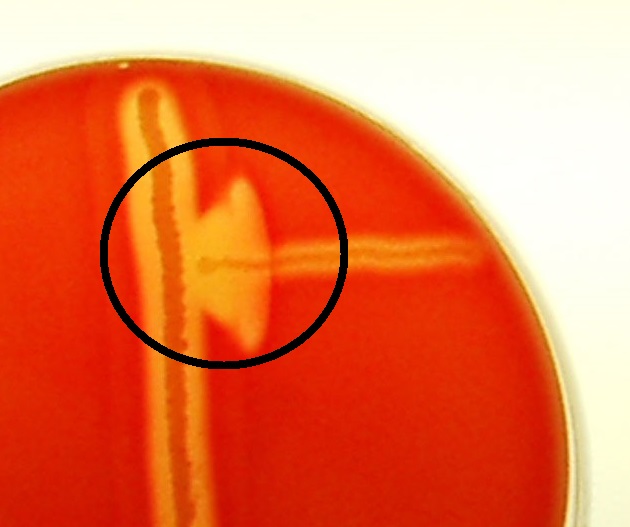
b. CAMP Test (Christie, Atkins, Munch–Petersen)
A positive CAMP reaction consisted of a semilunar-shaped area or circle of complete hemolysis of sheep erythrocytes and occurred only when colonies of group B streptococci developed along the periphery of the preformed zone of staphylococcal β-hemolysin.
3. Group C Streptococci
Group C streptococci (GCS) and Group G streptococci (GGS) are normal commensal flora of the human upper airway and frequently are asymptomatic colonizers of the skin, gastrointestinal tract, and female genital tract. Group C streptococci often has a very strong antiphagocytic hyaluronic capsule similar to that of group B streptococci.
Examples are Streptococcus dysgalactiae subsp. equisimilis (SDSE) & Streptococcus anginosus.
However, Streptococcus anginosus is now classified under the Streptococcus anginosus Group (SAG) or also known as Streptococcus milleri group which includes Streptococcus anginosus, Streptococcus intermedius, and Streptococcus constellatus.
4. Group D Streptococci
Group D streptococci (GDS) are indigenous in the gastrointestinal tracts of humans and animals. Currently, Streptococcus bovis, the most common GDS, has been re-classified into 4 different species (Streptococcus gallolyticus, Streptococcus pasteurianus, Streptococcus infantarius and Streptococcus lutetiensis).
Streptococcus bovis can cause disease, e.g., endocarditis, bacteremia, septic arthritis in compromised hosts and less frequently in healthy individuals. Bacteremia in patients with colonic neoplasia and bacterial endocarditis has been attributed primarily to S. bovis biotype I while biotype II (S. gallolyticus subsp. pasteurianus) has been associated with meningitis in both adults and infants.
The currently admitted classification based on Multilocus Sequence Typing (MLST) data defines seven subspecies:
Streptococcus
gallolyticus subsp. gallolyticus (Sgg)
Streptococcus
gallolyticus subsp. macedonicus (Sgm)
Streptococcus
gallolyticus subsp. pasteurianus (Sgp)
Streptococcus
infantarius subsp. infantarius (Sii)
Streptococcus
lutetiensis
Streptococcus
alactolyticus
Streptococcus equinus
Sgg is an opportunistic pathogen causing septicemia and endocarditis in elderly persons. Intriguingly, several clinical studies have demonstrated a strong association between invasive infections with Sgg and Colorectal Cancer (CRC) in humans although not the principal cause of but an auxiliary factor accelerating the development of CRC.
Streptococcus gallolyticus owes its name to its capacity to decarboxylate gallic acid, an organic acid derived from tannins hydrolysis.
Other disease produced by Streptococci:
1. Local infection – sore throat
2. Sepsis
3. SBE – Subacute Bacterial Endocarditis which is caused by viridans streptococci.
4. ABE – Acute Bacterial Endocarditis which is caused by Streptococcus pyogenes.
5. Scarlet Fever – a form of streptococcal pharyngitis caused by a strain of Streptococcus pyogenes.
Dick’s test – susceptibility test for scarlet fever, the test is done on the arm of the patient.
Schultz Charlton reaction or blanching phenomenon – diagnostic test for scarlet fever
6. Erysipelas or St. Anthony’s Fire
7. Impetigo contagiosa
Enzymes produced by Streptococci:
1. Streptokinase – involved in fibrinolysis; is given intravenously to patients suffering from pulmonary emboli and venous thrombosis; produced by beta hemolytic streptococci.
2. Streptodornase – liquefy exudates, thus it hastens removal of pus and necrotic tissue.
3. C5a peptidase – is a highly specific proteolytic enzyme that cleaves the complement–derived chemotaxin C5a. This protein aids in the evasion of the immune system by cleaving the chemotactic component of the complement cascade C5a. This protein has been studied in considerable detail, due its role in both pathogeneses, and as a potential vaccine candidate.
4. Hyaluronidase – aids in spreading of infection.
5. Diphosphopyridine nucleotidase – may kill leukocytes; proteinases and amylases are produced by some strains elaborating this enzyme.
Toxins produced by Streptococci:
1. Erythrogenic toxin or pyrogenic exotoxin – it is antigenic in nature which is destroyed by boiling for one hour and is responsible for skin rashes in scarlet fever.
a. Streptococcal Pyrogenic Exotoxin A (SPE A) is secreted by some strains of Streptococcus pyogenes and is strongly associated with streptococcal toxic shock syndrome (STSS), a severe and often fatal illness.
b. Streptococcal Pyrogenic Exotoxin B (SPE B) is an important streptococcal pyrogenic exotoxin in GAS infection. It is strongly associated with disease severity because of its proteolytic activities. It also causes severe inflammation in the host by activating interleukin 1β. It also inhibits the phagocytic activity of macrophages, but it is not clear what mechanism it uses to do this.
c. Streptococcal Pyrogenic Exotoxin C (SPE C) is a potent inducer of inflammatory cytokine production by T lymphocytes and is believed to play a key role in the pathogenesis of streptococcal toxic shock syndrome.
2. Hemolysin or streptolysin – elaborated by beta–hemolytic Group A streptococcus:
a. Streptolysin O (SLO) – belongs to a family of pore–forming, oxygen–labile, thiol–activated cholesterol–dependent cytolysins (CDCs) and causes the broad zone of beta hemolysis surrounding colonies of Group A Streptococcus (GAS) on blood agar plates. Exogenous cholesterol inhibits hemolysis both in vitro and in situations where serum cholesterol is high (e.g., nephrotic syndrome); thus, elevated antistreptolysin (ASO) titers occur because either cholesterol or anti–ASO antibody “neutralizes” SLO. CDCs are secreted, monomeric proteins that bind to eukaryotic cells and promote cytolysis through the formation of transmembrane pores.
The antibody, ASO, blocks hemolysis by Streptolysin O. The ASO serum titer more than 160 – 200 units indicates recent infection with streptococci with a high antibody level due to an earlier exposure in a hypertensive host.
b. Streptolysin S (SLS) – is a small (~2.8 kDa), non–immunogenic hemotoxin that is deposited upon the surface of target cells via direct Group A Streptococcus (GAS) contact and contributes to pathogenesis through inhibition of neutrophil opsonophagocytosis and modulation of the host immune response during early infection and responsible for the hemolytic zones produced by Streptococcus colonies on BAP.
|
DIFFERENCE
BETWEEN |
|
|
Streptolysin
O |
Streptolysin
S |
|
Antigenic |
Non–antigenic |
|
Oxygen labile |
Oxygen stable |
|
Responsible for subsurface hemolysis |
Responsible for surface hemolysis |
Laboratory diagnosis:
1. Stained smears – streptococcus appear as violet in strings.
2. Culture
|
Streptococcus
specie |
Culture
Media |
Colony
appearance |
|
Streptococcus pyogenes |
Columbia Agar with Colistin and Nalidixic Acid |
Green discoloration for alpha hemolysis, clear for
beta, and no change for gamma |
|
Horse Blood Agar with Polymyxin B sulphate,
Neomycin Sulphate and Fusidic acid |
Dome–shaped with a smooth or moist surface and
clear margins |
|
|
Streptococcus agalactiae |
Edwards Medium Base |
White grayish or opaque |
|
Streptococcus pneumonia (sputum) |
Crystal Violet–Nalidixic Acid–Gentamicin Agar
(CVNG) |
Small, flat, draughtsman type colonies with
greenish alpha hemolysis |
|
Group B Streptococci (GBS) |
Granada Medium (anaerobic) |
Red colonies |
|
Group A Streptococci (food sample) |
Colistin Crystal Violet Sulfamethoxazole
Trimethoprim (CCSXT) Agar |
|
|
Group D Streptococci (food sample) |
Kanamycin Esculin Azide Agar |
|
3. Serological test
a. ASO titer – increased when there is infection of any organ of the body, by Group A beta hemolytic streptococci (GABHS), Group C or Group G streptococci.
4. For Lancefield Grouping of Streptococcus species – uses antisera harvested from rabbit’s blood and carried out through Capillary Agglutination Test or Agar Gel Double Diffusion or Counterimmuno–electrophoresis.
DIPLOCOCCUS OR PNEUMOCCUS
Characteristics:
1. They are gram (+) cocci, lancet or flame–shaped, arranged in pairs or in short chains, encapsulated, non–motile, non–sporeformers.
2. They are facultative anaerobes that ferment carbohydrates with the production of lactic acid.
3. They do not produce the enzyme catalase or peroxidase, thus accumulation of H2O2 kills the organism unless catalase is provided in the culture medium.
4. For primary isolation, Brain Heart Infusion (BHI) agar, Trypticase Soy Agar (TSA) with 5% defibrinated sheep blood is employed. Candle jar method or CO2 incubator is used for cultivation.
Young colonies are dome–shaped but on aging, becomes flattened with a raised margin and depressed center resembling “checker” or nail–head appearance with greenish discoloration (alpha–hemolysis). The alpha hemolysis of the streptococci is indistinguishable from the alpha hemolysis produced by the pneumococci. Certain tests must be done to differentiate one from the other.
Disease produced:
1. Lobar
pneumonia
2. Meningitis
3. Septicemia
4. Otitis
media
Antigenic Structure:
1. Soluble Specific Substance (SSS) – a polysaccharide capsular substance which determines the virulence of the pneumococci, rendering it resistant to phagocytosis. This is also used as a basis for serologic typing of pneumococcal strains.
2. Somatic
antigen
– the C–antigen precipitated by the C–reactive protein in the serum of patients
with pneumococcal infection.
Pathogenic factors:
1. Pneumolysin (PLY) – properties similar to Streptolysin O. It is a cholesterol–dependent cytolysin (CDC) and key pneumococcal virulence factor involved in all phases of pneumococcal disease, including transmission, colonization, and infection.
2. Neuraminidase (NanA) – contributes to the invasiveness of the organism. It acts on the glycoprotein in cell membrane and body fluids. It also provides a source of carbohydrates for bacterial metabolism, cleaving sugars from the mucosal surface.
|
TEST
DIFFERENTIATING PNEUMOCOCCI FROM STREPTOCOCCI |
||
|
|
Pneumococci |
Streptococci |
|
Bile Solubility Test |
Soluble |
Insoluble |
|
Inulin Fermentation |
Fermenter |
Non–fermenter |
|
Capsular swelling |
Swelling |
No swelling |
|
Quinidine |
Susceptible |
Resistant |
|
Optochin Test |
Susceptible |
Resistant |
|
Mouse Virulence Test |
Mouse dies within 16 – 48 hours |
Mouse don’t die |
Laboratory Diagnosis:
1. Bile Solubility Test – bile (Ox bile or 10% sodium taurocholate) acts upon the cell wall of pneumococci bringing about lysis. The test is best on the presence of an autolytic amidase in pneumococci which is activated by bile leading to the dissolution of organisms. Bile solubility is demonstrated by the clearing or loss of turbidity in the "test" tube relative to "control" tube.

2. Optochin growth inhibition test – the most widely used test to differentiate pneumococci from other alpha hemolytic streptococcus. Optochin disc is composed of ethyl hydrocupreine and hydrochloride.

3. Mouse virulence test – an animal inoculation test that measures the survival of mouse against varying dose of colonies of Pneumococcus.

4. Capsular swelling test or Neufeld Quellung reaction – most accurate, reliable, specific test for identifying pneumococci.
.jpg)
5. Inulin Fermentation Test – inulin is the only carbohydrate fermented by pneumococci.

6. Francis Test – an obsolete susceptibility test for pneumococcal infection. Susceptibility denotes the absence of circulating antitoxin in the blood.
THE GRAM–POSITIVE ANAEROBIC COCCI
Gram-positive anaerobic cocci (GPAC) are part of the normal flora of all mucocutaneous surfaces and are often isolated from infections such as deep organ abscesses, obstetric and gynecological sepsis, and intraoral infections. Large numbers of GPAC can be found in the female genitourinary tract; counts vary with physiological processes such as the stage of the menstrual cycle and pregnancy. They can be cultured from a wide variety of sites, particularly abscesses and infections of the mouth, skin and soft tissues, bone and joints, and upper respiratory and female genital tracts. GPAC were the most common anaerobic group isolated from patients with cellulitis, necrotizing fasciitis, mediastinitis, pyomyositis, pediatric bite wounds, anaerobic conjunctivitis associated with contact lenses, post-thoracotomy sternal wound infections, and external otitis.
Watt and Jack defined anaerobic cocci as “cocci that grow well under satisfactory conditions of anaerobiosis and do not grow on suitable solid media in 10% CO2 in air even after incubation for 7 days at 37°C.” Most GPAC are resistant to sodium polyanethol sulfonate (SPS; Liquoid) except for Peptostreptococcus anaerobius.
The most used culture media is the Nalidixic Acid-Tween Blood Agar and the Fastidious Anaerobe Agar.
Members of the group are:
1. Peptostreptococcus
Cells vary in size from 0.3 to 2.0 μm and can be arranged in chains, pairs, tetrads, or clumps; most species are present either as chains or clumps. They do not form spores. For most species, the products of protein digestion appear to be the principal energy source.
Peptostreptococcus anaerobius was the only representative of the genus until Peptostreptococcus stomatis was recently described. Peptostreptococcus anaerobius in a broad sense has been frequently cultured from clinical specimens from the mouth, upper respiratory tract, skin and soft tissues, bone and joints, and gastrointestinal and genitourinary tracts. It’s been suggested that the novel species, Peptostreptococcus stomatis, originates from the oral cavity, whereas Peptostreptococcus anaerobius sensu stricto has its habitat and is involved in infections under the waistline.
Peptostreptococcus magnus has been recovered in pure culture from a range of serious infections, some of which have been fatal; reports have described cases of native-valve endocarditis, paravalvular abscess round a bioprosthetic aortic valve, purulent pericarditis complicated by mediastinitis, meningitis after neurosurgery, and anaerobic necrotizing pneumonia complicated by pyopneumothorax. It is the predominant anaerobe in investigations of nonpuerperal breast abscesses and diabetic foot infections; peripheral infections secondary to vascular disease frequently progressed to osteomyelitis. It has a strong association with soft tissue infections, particularly wound infections and superficial abscesses, in which it is often present in pure culture.
2. Peptococcus (Peptococcus niger)
It forms black colonies on blood agar on initial culture of fresh isolates but became grey on exposure to air; after several laboratory transfers, cultures from blood agar plates no longer produced pigment.
Its most distinctive feature is its VFA profile, which includes acetic, isobutyric, butyric, isovaleric, and terminal n-caproic acids.
3. Ruminococcus
The cell morphology can be ovoid or spheroid, with ends that can be flat, rounded, or pointed, depending on the species; unlike sarcinae, cells are arranged in pairs or chains and do not form spores; many strains retain Gram’s stain poorly and therefore appear gram negative. Ruminococci are strongly saccharolytic; most species require carbohydrates for growth, do not utilize peptides, and use ammonia as their nitrogen source. The ability to digest cellulose may be an important marker. The major volatile fatty acid (VFA) formed is acetic acid, which distinguishes them from coprococci.
4. Coprococcus
The genus Coprococcus was proposed for novel organisms isolated in an investigation of the fecal flora. The new genus comprised species of nonsporing GPAC for which fermentable carbohydrates were required or highly stimulatory and which formed butyric acid as their terminal VFA.
The genus has a G+C content of 39 to 42 mol%; the type species is Coprococcus eutactus. Coprococci are unlikely to grow in commercial media. The three species, Coprococcus eutactus, Coprococcus comes, and Coprococcus catus, were originally described from the human gastrointestinal tract but have not yet been reported from clinical specimens.
5. Sarcina
The genus
Sarcina is unique because the cell morphology reveals gram–positive cocci
characteristically arranged in packets of eight which can form spores. Sarcinae
are strict anaerobes that require fermentable carbohydrates; they will grow in
a pH range between 1 and 9.8.
THE ENTEROCOCCI
Characteristics:
1. They typically have an optimum growth temperature of 35°C and a growth range from 10 to 45°C.
2. They typically grow in broth containing 6.5% NaCl and hydrolyze esculin in the presence of 40% bile salts.
3. They are catalase reaction negative, and do not express complete cytochromes, although some species produce a catalase and appear catalase positive with weak effervescence.
4. They are usually homofermentative, producing lactic acid as the end product of glucose fermentation, without production of gas.
5. Pigmentation varies in different species.
6. They are often used for the preparation of traditional cheeses manufactured in Mediterranean countries because of their natural occurrence as contaminants of raw meat and dairy products, thermotolerance, low toxicity, and their ability to acidify an environment, they have become an important ingredient in fermented foods (but not as probiotics).
7. Virulence factors include structural durability, bacteriocins, hemolysin/cytolysin, gelatinase (a serine protease), and biofilm production. Antibiotic resistance is intrinsic or acquired through the transfer of resistance-related mobile genetic elements (MGE) via various mechanisms like plasmids, conjugation, and transposons.
8. They are indicators of the presence of fecal material in water and, therefore, of the possible presence of disease-causing bacteria, viruses, and protozoa.
9. They are commensal bacteria in the intestines of humans and domestic animals, but they can also be detected in the environment, from soil, water, plants, wild animals, birds, and insects. They can cause infection only when introduced to other sites.
10. The two enterococcal species that are most pathogenic to humans, E. faecalis and E. faecium, showed the greatest resistance to desiccation and starvation. These two species also show high levels of resistance to the common hospital disinfectants chloroxylenol and chlorhexidine.
11. In humans, Enterococcus faecalis and Enterococcus faecium can cause urinary tract infections, wound infections, bacteraemia, and infective endocarditis.
Classification of Enterococci:
1. Group I consist of enterococcal species that form acid in both carbohydrate broths, but do not hydrolyze arginine.
2. Group II includes species that form acid in mannitol broth and hydrolyze arginine but fail to form acid in sorbose broth and unable to use raffinose (raffinose utilization is a trait carried by megaplasmids, which indicates that these mobile elements can have important roles in shaping the competitive fitness of the enterococci in the environment; for example, by expanding their metabolic repertoire). Pathogenic strains to humans like E. faecalis and E. faecium belong to this group.
3. Group III includes species that are not able to form acid in either mannitol or sorbitol broth, but that hydrolyze arginine.
4. Group IV, these species are negative for acid formation in mannitol and sorbose broth and do not hydrolyze arginine.
5. Group V consists of the species that form acid on mannitol, but not sorbose broth, and fail to hydrolyze arginine.
Enterococcus faecium
1. Part of the ESKAPE bacteria group which are a group of opportunistic pathogens consisting of Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species characterized by increased levels of resistance towards multiple classes of first line and last–resort antibiotic.
2. The specie is resistant to Vancomycin antibiotic termed as “Vancomycin– resistant Enterococcus (VRE).”
3. Enterococcus faecium species are 80% vancomycin-resistant and 90% ampicillin-resistant compared to Enterococcus faecalis species, which are only 10% vancomycin-resistant and mostly ampicillin sensitive.
4. They ferment arabinose as a nutrient source.
Enterococcus faecalis
1. Highly virulent strains of E. faecalis express a pore-forming exotoxin, called cytolysin (aka Enterolysin A), which lyses both bacterial and eukaryotic cells in response to quorum signals.
2. They are the third most isolated healthcare pathogen.
3. They ferment mannitol as a nutrient source.
Culture:
There are numerous culture media available to isolate Enterococcus due to its presence in surface water or food or meat products. Listed below are the ones commonly employed in a clinical setting.
1. Bile Esculin Azide Agar
Bile Esculin Azide Agar is a selective medium used for isolation and presumptive identification of fecal Streptococci.
It is based on the principle that Enterococci can hydrolyze esculin into esculetin and glucose. The reaction between esculetin and ferric ammonium citrate results in a brown black to black halo around the colonies. Ox bile inhibits the growth of gram–positive bacteria except enterococci, while sodium azide suppresses the gram–negative bacteria.
2. Thallous Acetate Tetrazolium Glucose (TITG) agar
The differentiation is based upon the reduction of tetrazolium. Enterococcus faecalis produces colonies with a deep red center and a narrow white periphery, whereas Enterococcus faecium produces white or pale pink colored colonies.
3. Mitis Salivarius Agar
A medium used with supplements for the selective isolation of Streptococcus viridans, such as Streptococcus mitis and Streptococcus salivarius, and Enterococcus faecalis, from specimens containing mixed microbial flora. Enterococcus usually form dark blue or black colonies on this agar plate.
Some of the added supplements of the agar includes the addition of tellurite or bacitracin depending on the species to be isolated or the type of specimen (e.g., saliva) to be used.
4. Mannitol Salt Agar (MSA)
Enterococcus faecalis can grow on MSA and ferment mannitol whereas Enterococcus faecium does not.
5. Cephalexin–Aztreonam–Arabinose Agar (CAA)
Enterococcus faecium can grow on CAA and ferment arabinose whereas Enterococcus faecalis do not.
THE AEROCOCCI
Characteristics:
1. Aerococcus species is a Gram–positive, catalase–negative and oxidase–negative, microaerophilic, alpha–hemolytic, non–motile bacteria often confused with streptococci species or treated as a contaminant.
2. Five species have been identified as pathogenic in humans, with a spectrum of diseases ranging from urinary tract infections (UTI), bloodstream infections (BSI), and endocarditis to spinal infections.
Aerococcus
urinae
Aerococcus
viridans
Aerococcus
sanguinicola
Aerococcus
urinaehominis
Aerococcus christensenii (vaginal tract)
3. They can be found in a very small number as indigenous inhabitants in the upper respiratory tract and on the skin of normal persons. This organism is generally saprophytic and has rarely been encountered as a human pathogen.
4. They are best identified using MALDI–TOF MS (Matrix–assisted Laser Desorption Ionization Time–of–Flight Mass Spectrometry).
Aerococcus urinae is a bacterium of emerging clinical interest that most commonly causes urinary tract infections (UTI) but can also result in invasive infections. It is a catalase–negative, alpha–haemolytic gram–positive coccus that grows in clusters or tetrads and usually causes urinary tract infections.
Aerococcus urinae can, in older males with underlying urinary tract conditions, cause invasive infections such as urosepsis or infective endocarditis.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.